Visual answer
How Eye Drops Work: the idea in one diagram
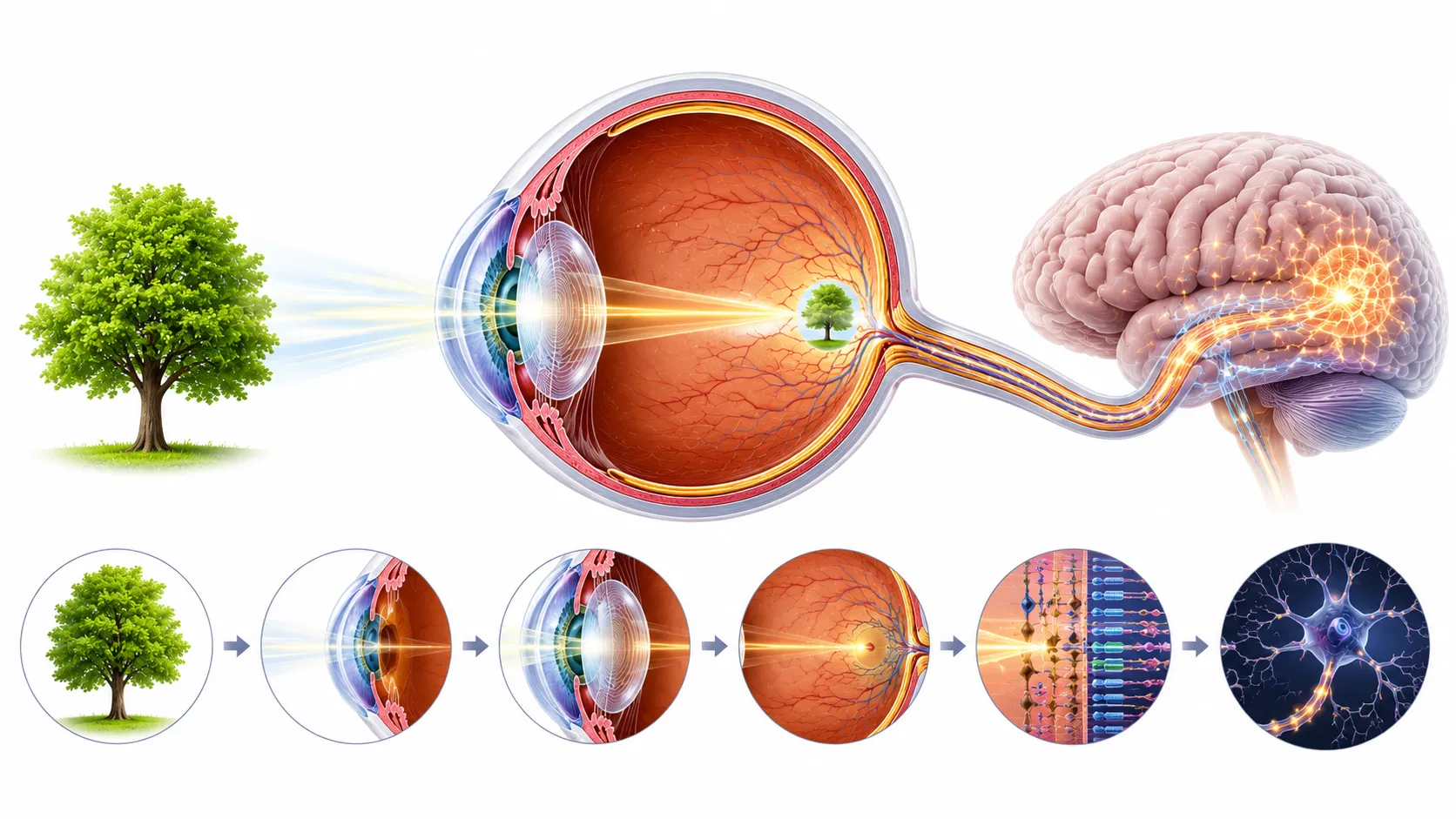
An eye drop must land on the tear film, survive overflow and blinking, avoid rapid drainage, and cross the cornea's layered chemical barriers before it can treat internal eye tissue.
The drop lands on the tear film
The eye can hold only a fraction of a standard drop.
Most fluid drains away
Drainage explains both waste and the bitter throat taste.
The drug crosses the cornea
Eye drop chemistry determines how much reaches the target.
Answer
The Direct Answer
Eye drops work by depositing a drug onto the ocular surface, from which it must penetrate the cornea to reach internal eye structures. Most of the drop washes away through the nasolacrimal duct, which is why you can taste it.
When a drop lands on the eye, it joins the tear film. The eye can hold approximately seven to ten microliters of fluid. A standard drop contains about thirty microliters, meaning most of it immediately overflows and drains through the puncta, tiny holes in the inner corners of the eyelids, down the nasolacrimal duct, and into the back of the throat. The remaining drug must cross the cornea, a selective barrier with tight cellular junctions, to reach the anterior chamber where most ocular conditions are treated.
The eye is extraordinarily well-defended against anything entering it, including the medication you are deliberately trying to put there. Understanding the obstacles is more interesting than the solution.
Big questions
The Questions That Make It Interesting
These are the pressure points of the idea: the places where the simple answer becomes a much stranger story.
Why do eye drops taste in your throat?
Because the nasolacrimal duct, the drainage channel for tears and excess ocular fluid, empties into the nasal passage, which connects to the throat. Drug absorbed through the highly vascular nasal mucosa reaches the bloodstream, and drug that travels further reaches taste receptor areas in the posterior nasal and pharyngeal space.
The eye, the nose, and the throat are pharmacologically connected in a way most people never realize until they taste their own eye drops.
Why is the cornea such an effective drug barrier?
The cornea has three main layers with different chemical properties. The outer epithelium is lipophilic, preferring fat-soluble compounds. The middle stroma is hydrophilic, preferring water-soluble ones. The inner endothelium is lipophilic again. A drug must have the right balance of fat-solubility and water-solubility to cross all three layers in sequence.
The cornea has essentially evolved a passport control that checks lipid and water solubility at three separate checkpoints.
Could you ever design a drop that gets more than five percent into the eye?
Yes, and this is an active area of pharmaceutical research. Viscosity-enhancing agents slow drainage. Nanoparticle carriers improve corneal penetration. Mucoadhesive polymers help the drop stick to the ocular surface longer. Contact lens-based delivery systems that sit on the eye and release drug slowly have shown dramatically higher bioavailability in clinical trials.
The entire field of ocular drug delivery is essentially a multi-billion dollar engineering effort to outmaneuver an evolutionary mechanism the eye developed to expel foreign substances.
Surprises
The Surprising Details
Surprising fact
A standard eye drop contains roughly three times more fluid than the eye can physically hold, meaning most of the dose is waste by design.
Surprising fact
Closing your eyes for two minutes after instilling eye drops and pressing gently on the inner corner dramatically reduces systemic absorption and improves ocular bioavailability.
Surprising fact
Some eye drop drugs can produce systemic effects significant enough to affect blood pressure, heart rate, or blood glucose because the nasolacrimal route delivers them directly to highly vascularized nasal mucosa.
Counterintuitive finding
Bigger drops do not work better. The eye's holding capacity is fixed. Extra volume simply overflows faster.
Counterintuitive finding
Blinking aggressively after instillation pumps the drug away from the eye more rapidly through the drainage system.
Counterintuitive finding
Some of the most serious side effects of common glaucoma drops, including bradycardia and bronchospasm, occur because the drug enters the bloodstream through nasal absorption, not the eye itself.
Fascinating comparison
Delivering a drug via eye drop is like watering a single plant in a garden by turning on the entire sprinkler system. The target gets wetted, but most of the water lands elsewhere.
Fascinating comparison
The cornea is selective about what crosses it in the same way a nightclub bouncer is selective about who enters: too hydrophilic and you are turned away, too lipophilic and you are also turned away, the chemistry has to be exactly right.
Everyday example
Beta-blocker eye drops used for glaucoma have been known to cause breathing difficulties in asthmatic patients because absorbed drug reaches lung tissue through systemic circulation.
Everyday example
The bitter taste experienced after using certain antibiotic eye drops is drug absorbed through the nasal mucosa reaching taste receptors.
Mechanism
How It Actually Works
An eye drop must land on the tear film, survive overflow and blinking, avoid rapid drainage, and cross the cornea's layered chemical barriers before it can treat internal eye tissue.
- 1
The drop lands on the tear film
The medication first mixes with the thin tear layer covering the cornea and conjunctiva. Analogy: A bucket of water poured onto a small sponge. Takeaway: The eye can hold only a fraction of a standard drop.
- 2
Most fluid drains away
Extra fluid overflows or passes through the puncta into the nasolacrimal duct, then toward the nose and throat. Analogy: A sink with an open drain beside the target. Takeaway: Drainage explains both waste and the bitter throat taste.
- 3
The drug crosses the cornea
The remaining drug must pass through lipid-loving and water-loving corneal layers in sequence. Analogy: Three passport checks with different entry rules. Takeaway: Eye drop chemistry determines how much reaches the target.
Story
The Story Behind the Science
The Glaucoma Treatment That Changed Cardiology
When timolol, a beta-blocker, was introduced as an eye drop for glaucoma in the late 1970s, ophthalmologists began reporting unexpected cardiovascular and respiratory side effects. Patients were experiencing bradycardia and bronchospasm from a drug applied topically to the eye.
It demonstrated that the eye is not pharmacologically isolated from the rest of the body and forced a revision of how systemic absorption from eye drops was monitored. A drug delivery route that seemed local turned out to be systemic, and the consequences were severe enough to change prescribing practice.
Introduction of pilocarpine eye drops for glaucoma, 1870s
Pilocarpine became one of the first drugs deliberately formulated as an eye drop to treat elevated intraocular pressure, marking the beginning of modern topical ocular pharmacology.
It established both the potential and the limitations of eye drop delivery: effective for surface and anterior segment conditions but constrained by the eye's natural defense and drainage systems.
Evidence
Experiments and Evidence
Nasolacrimal occlusion studies, 1970s and 1980s
Researchers demonstrated that pressing gently on the puncta after instilling eye drops significantly reduced systemic absorption and measurably increased the drug's duration in the eye.
A technique requiring no additional equipment or medication, just a finger pressed to the inner eye corner for two minutes, could double or triple the effective dose reaching the target tissue.
Pattern
The Deeper Pattern
The eye blinks approximately fifteen to twenty times per minute, partly to spread the tear film but also, from a drug delivery perspective, to actively pump most of your eye drop down the drain.
The blink reflex evolved to protect the eye from foreign objects. It does this job with devoted indifference to whether the foreign object is bacteria or expensive glaucoma medication.
Timolol eye drops for glaucoma can cause bronchospasm in asthmatic patients, clinically significant drops in heart rate, and even depression, all because the nasolacrimal route delivers the drug into systemic circulation.
A drop placed in the eye for a pressure problem in the eyeball can affect breathing and mood through a plumbing route in the face that most patients do not know exists.
Eye drop pharmacology illustrates a principle that applies far beyond medicine: the most direct route is rarely the most efficient one, and the target's own defenses often work against the very interventions meant to help it.
The eye's elaborate defense systems, the tear film, the drainage ducts, the corneal barriers, all evolved to exclude foreign material. Medicine cannot simply override these systems. It must negotiate with them.
Effective intervention requires understanding a system's defenses well enough to work with them rather than against them.
Edge cases
Where the Rule Gets Weird
Eye drops in pediatric patients.
Because children have lower body weights, the proportion of a systemically absorbed eye drop dose relative to body mass is much higher than in adults.
The same drop that is unremarkable in an adult glaucoma patient becomes a dosing challenge in a child, simply because the systemic compartment is so much smaller.
Myths
Myths vs Reality
Eye drops stay in the eye and work locally.
A significant fraction of most eye drop doses enters the systemic circulation via nasolacrimal drainage, meaning eye drops can produce body-wide drug effects.
Measurable plasma concentrations of eye drop drugs have been documented for beta-blockers, prostaglandin analogues, and antibiotics following standard topical instillation.
Using more drops more often improves treatment.
Exceeding recommended drop frequency rarely improves therapeutic effect and may increase systemic side effects by delivering more drug to the nasolacrimal drainage system.
Corneal uptake reaches saturation quickly. Additional drops simply pass through drainage channels rather than penetrating ocular tissue.
Real world
What This Changes in Real Life
The simple technique of punctal occlusion, pressing on the inner corner of the eye for one to two minutes after instilling drops, meaningfully improves the efficacy of glaucoma and other long-term ocular medications while reducing systemic side effects.
Studies have shown punctal occlusion reduces systemic timolol absorption by up to 70 percent, potentially eliminating systemic side effects in sensitive patients while maintaining therapeutic intraocular pressure control.
Takeaways
Key Takeaways
Takeaway 1
A standard eye drop is about three times larger than the eye can hold, so most overflows immediately.
Takeaway 2
Less than five percent of a typical eye drop reaches its target tissue inside the eye.
Takeaway 3
Drug draining through the nasolacrimal duct enters the bloodstream and can cause systemic side effects.
Takeaway 4
Pressing on the inner eye corner for two minutes after drops dramatically improves their effectiveness.
Takeaway 5
Eye drop drug chemistry must be calibrated to cross the cornea's triple-layer lipid-hydrophilic-lipid barrier.
Quick answers
Common questions
Why do eye drops taste in your throat? +
Because the nasolacrimal duct, the drainage channel for tears and excess ocular fluid, empties into the nasal passage, which connects to the throat. Drug absorbed through the highly vascular nasal mucosa reaches the bloodstream, and drug that travels further reaches taste receptor areas in the posterior nasal and pharyngeal space.
Why is the cornea such an effective drug barrier? +
The cornea has three main layers with different chemical properties. The outer epithelium is lipophilic, preferring fat-soluble compounds. The middle stroma is hydrophilic, preferring water-soluble ones. The inner endothelium is lipophilic again. A drug must have the right balance of fat-solubility and water-solubility to cross all three layers in sequence.
Could you ever design a drop that gets more than five percent into the eye? +
Yes, and this is an active area of pharmaceutical research. Viscosity-enhancing agents slow drainage. Nanoparticle carriers improve corneal penetration. Mucoadhesive polymers help the drop stick to the ocular surface longer. Contact lens-based delivery systems that sit on the eye and release drug slowly have shown dramatically higher bioavailability in clinical trials.